63 yr old male with c/o facial puffiness and fever
Hi , I am Indu Vaishnavi, 5th semester medical student. This is an online e log of patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.This elog also reflects my patient centered online learning portfolio
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan
63 yr old male from pedhevulapalli came to OPD 5 days ago with
c/o-swelling of face and legs since 1 month
Fever (on and off)since 2 months
HOPI:
Patient was apparently asymptomatic 2yrs back.Then he had an attack of left hemiparesis.First he developed stiffness in his left wrist and then he developed stiffness in his left hand and left leg he has no sensation in his left limb.He immediately reached out to the hospital in miryalaguda and treatment was given accordingly.
From then he is on clopidogril and calcium tablets.
After this attack he complains of decrease of power in his left upper and lower limbs.
After few days of this attack he developed black patches on his hands, abdomen and legs,and then progressed to all over body. Associated with itching and scaling during nights mostly.He has burning and pricking sensation,relieved by medication
No h/o seasonal variation of itching.H/o of application of luvicinazole,miconazole,clobeterol, salicylic acid, liquid paraffin with no improvement .
He gives a history of fever (on and off) associated with chills(morning) and rigors, relieved on medication.
Past history:
No h/o of similar complaints in the past .
He gives a history of joint pains of hand and feet not associated with morning sickness.
He had an trauma in his left knee 7yrs ago and he was not treated and condition gradually worsened.
He is k/c/o hypertension since 2 yrs
N/k/c/o Diabetes ,leprosy,thyroid,asthma,CAD
Treatment history:
He is on medication for hypertension
since 2yrs.
He is on clopidogril and calcium tablets
since 2 yrs.
Personal history:
He is married, sedentary lifestyle
Normal appetite,vegetarian(stopped non veg since 2yrs)
Normal bowels and normal micturition
No known allergies
He used to consume toddy occasionally from past 2 yrs he has stopped it
No other addictions
GENERAL EXAMINATION
In a well lit and adequately ventilated room with proper consent from patient's informant general examination was done
And patient was
Conscious and coherent
No pallor, icterus, cyanosis, clubbing of fingers, lymphadenopathy
In a well lit and adequately ventilated room with proper consent from patient's informant general examination was done
And patient was
Conscious and coherent
No pallor, icterus, cyanosis, clubbing of fingers, lymphadenopathy
Pedal edema is seen

SYSTEMIC EXAMINATION
CVS
S1 & S2 heard, no murmurs
RESP
Inspection- flat chest with a slight depression in the centre
Palpation - bilateral air entry present, normal vesicular breath sounds heard, no adventitious sounds
ABDOMEN
soft non tender , umblicus is everted, no scars and sinuses.
CVS
S1 & S2 heard, no murmurs
RESP
Inspection- flat chest with a slight depression in the centre
Palpation - bilateral air entry present, normal vesicular breath sounds heard, no adventitious sounds
ABDOMEN
soft non tender , umblicus is everted, no scars and sinuses.
SYSTEMIC EXAMINATION
CVS
S1 & S2 heard, no murmurs
RESP
Inspection- flat chest with a slight depression in the centre
Palpation - bilateral air entry present, normal vesicular breath sounds heard, no adventitious sounds
ABDOMEN
soft non tender , umblicus is everted, no scars and sinuses.
CVS
S1 & S2 heard, no murmurs
RESP
Inspection- flat chest with a slight depression in the centre
Palpation - bilateral air entry present, normal vesicular breath sounds heard, no adventitious sounds
ABDOMEN
soft non tender , umblicus is everted, no scars and sinuses.
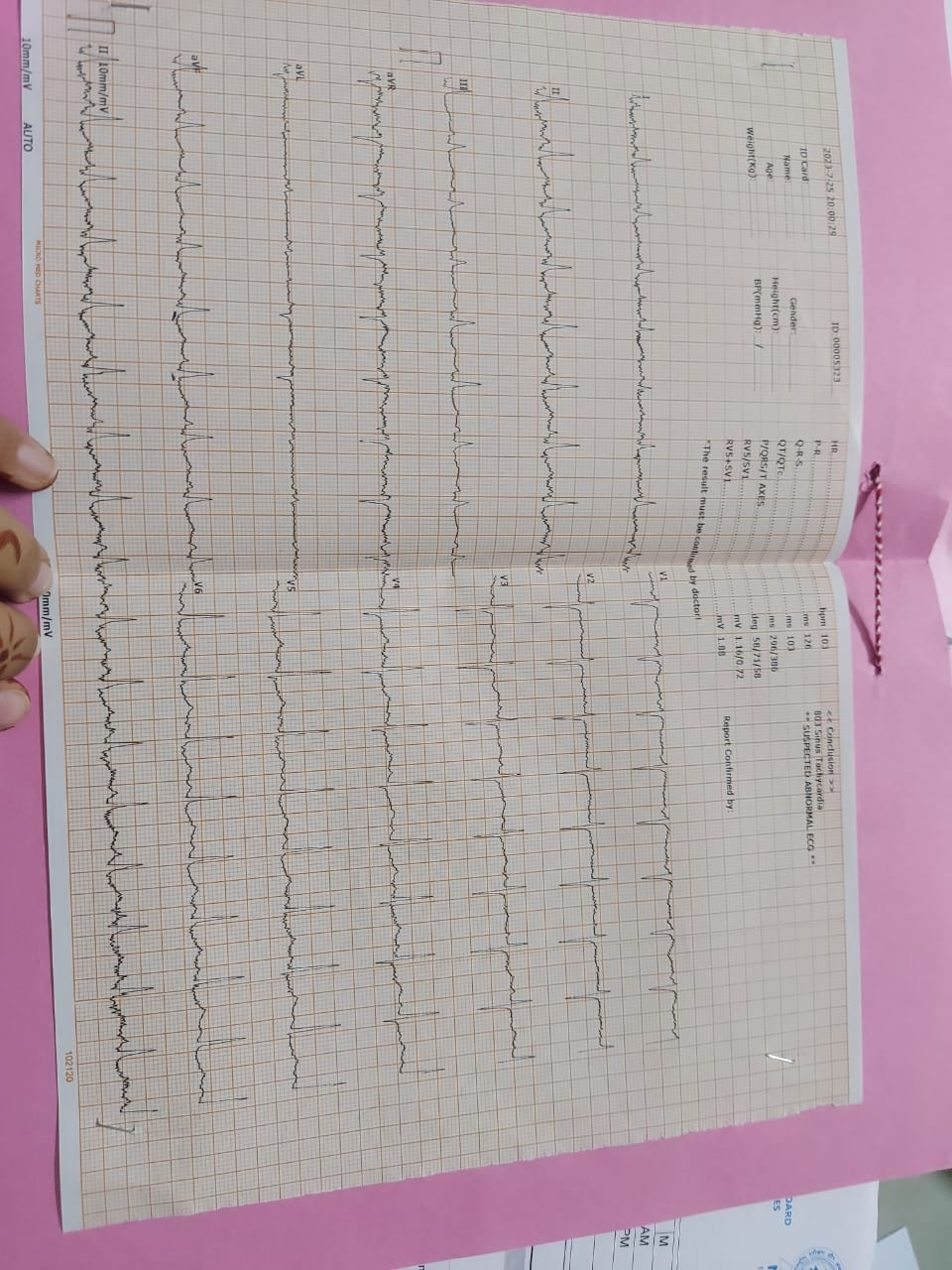
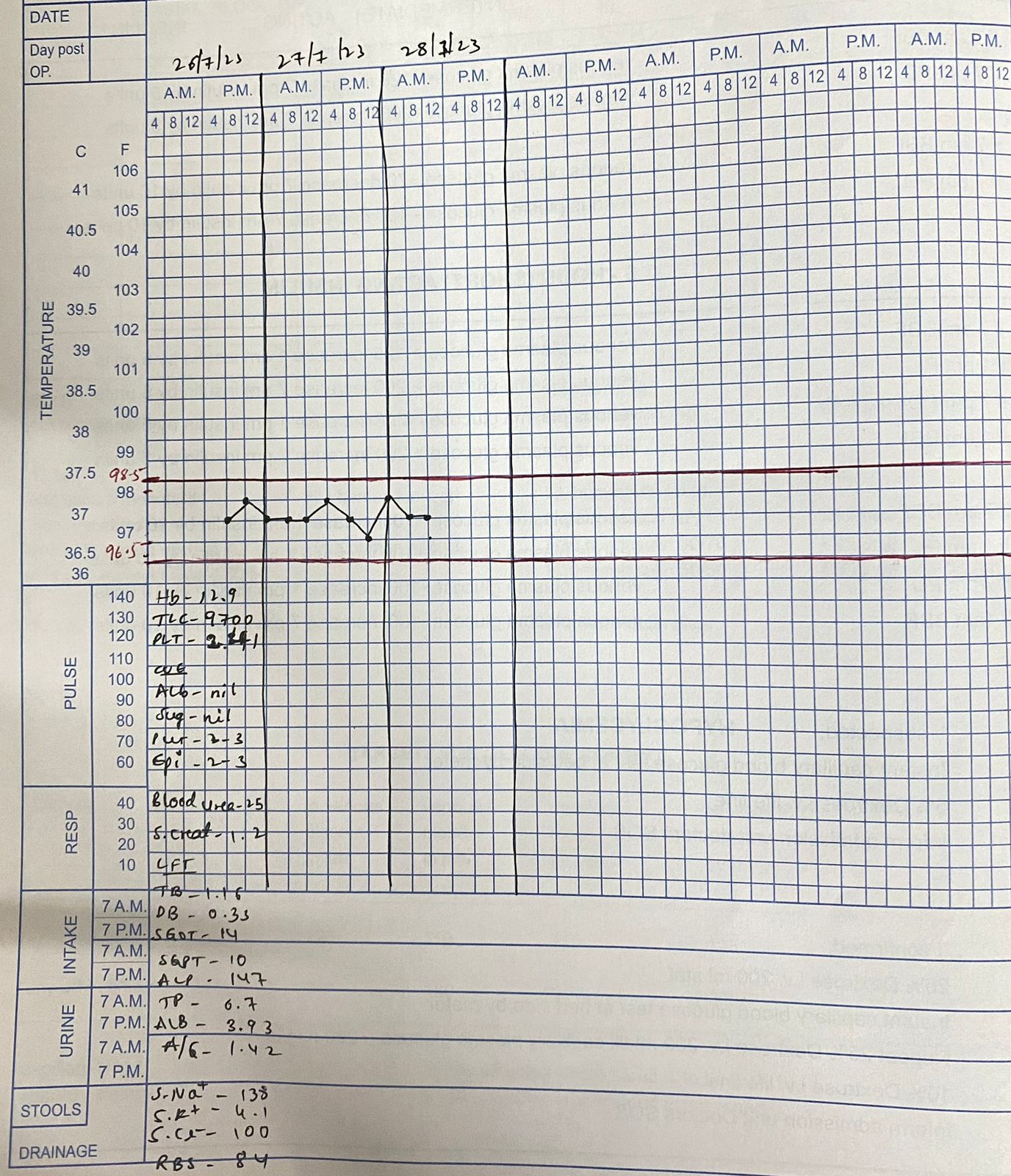
Investigations:










Comments
Post a Comment