60 YO MALE WITH BURNING MICTURATION, INCREASED FREQUENCY AND UNCONTROLLED SUGARS
60 YO MALE WITH BURNING MICTURATION, INCREASED FREQUENCY AND UNCONTROLLED SUGARS
Hi , I am Indu Vaishnavi, 5th semester medical student. This is an online e log of patient's de-identified health data shared after taking his/her/guardian's signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.This elog also reflects my patient centered online learning portfolio
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan
A 60 YO male, a resident of Nalgonda district came to the hospital with the chief complaints of:
- Difficulty in passing urine
- Burning micturation
- Abdominal pain
HOPI:
Patient was apparently asymptomatic 3 years back when he developed a fever for which the patient visitted a local hospital and was diagnosed with Type 2 diabetes mellitus and was put on oral hypoglycemic drugs, which he has been taking regularly.
H/o trauma due to fall from lorry 5 years back
2 years ago the patient started having gangerene and autoamputation of the fingers of his left hand.
3 months ago the patient went to a local hospital to get a check up, where it was found that his blood sugar levels were uncontrolled and was put on insulin to control the same.
3 months ago the patient started having complaints of difficulty in passing urine, increased frequency of micturation, burning micturation.
Abdominal pain since 3 months in the hypogastric area, intermittant, non radiating, squeezing type. No releiving or aggrevating factors.
Pt complaints of inability to retract foreskin.
PAST HISTORY:
No similar complaints in the past.
K/C/O: Type II DM since 3 years.
N/K/C/O HTN, TB, CAD, CVA, Asthma, Thyroid disorders.
SURGICAL HISTORY:
No relavent surgical history
PERSONAL HISTORY:
Diet: Mixed
Appetite: Normal
Sleep: Normal
Bowel: regular
Bladder: Difficulty in micturating, burning micturation
Habits: consumed alcohol regularly from 20 years of age. 2-3 drinks a day. Stopped 2 months ago.
SOCIAL HISTORY AND DAILY ROUTINE:
The patient attended school till third grade.
Until 3 years ago the patient worked as a daily wage worker but stopped working 3 years ago after he was diagnosed with diabetes.
He now wakes up at around 6 am, has 'Jonna Annam' for breakfast at around 7-8 am. He has white rice with curry for lunch at around 1pm. He has jowar roti with curry for dinner at around 8 pm and goes to bed by 9 pm.
He occupies his time by socializing with his freinds and neighbours.
GENERAL EXAMINATION:
The patient was examined after taking consent in a well lit room.
The patient was conscious, coherent and cooperative.
He is mederately built and nourished.
Pallor: Present
Icterus: Absent
Cyanosis: Absent
Clubbing: Absent
Lymphadenopathy: Absent
Edema: Absent




Vitals:
PR: 80 BPM
RR: 16 cpm
BP: 110/70mmHg
SpO2: 98%
Temperature: 98.4°F
SYSTEMIC EXAMINATION:
CVS:
On inspection:
Precordium is normal
Apex impulse could not be seen
No visible pulsations
On palpation:
Apex beat localised to 5th intercostal space medial to mid clavicular line.
No parasternal heave
No palpable thrills
On auscultation:
S1 and S2 heard.
No cardiac murmurs heard.
RS:
On inspection:
Chest shape is elliptical
Exapands equally on inspiration
Trachea: central
On palpation:
Tactile vocal fremitus is equal in all areas
On percussion:
Resonant note on all regions.
On auscultation:
Bilateral air entry positive
Vesicular breath sounds are heard.
No adventitious sounds such as crepts, rochi, etc heard.
ABDOMEN:
On inspection
Abdomen is scaphoid.
Umbulicus is central and inverted
No scars or sinuses
On palpation:
Abdomen is soft
No tenderness
No organomegally.
On auscultation:
Bowel sounds heard.
CNS:
Cerebellar functions normal.
Cranial nerve examination normal.
Sensory examination: sense of fine touch decreased in b/l lower limbs, coarse touch is normal.
Motor examination:
R. L
Tone:
UL. N. N
LL. N. N
Power:
UL. 5/5 5/5
LL. 5/5 5/5
Reflexes:
Biceps. +. +
Triceps. +. +
Knee. +. +
Ankle. - -
Babinski. Flexor. Flexor
INVESTIGATIONS:

ECG ON 26/7/23

USG ABDOMEN AND PELVIS ON 26/7/23

ABF ON 28/7/23 AT 4PM

2D ECHO ON 26/7/23

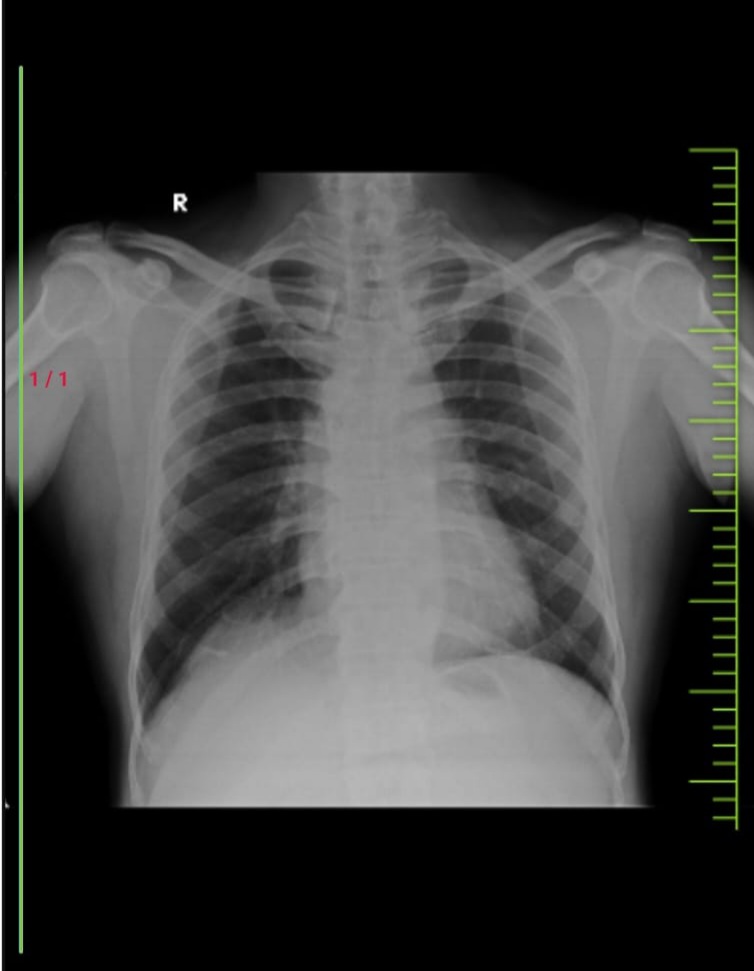
CXR PA VIEW

29/7/23

29/7/23
GRBS AND INSULIN CHART:

From 28/7/23
PROVISIONAL DIAGNOSIS:
Balanoposthitis with BPH with ?AKI ON CKD III with uncontrolled sugars with DM type 2 since 3 years.TREATMENT:
Strict diabetic diet
T. Augumentin 625 mg PO BD
T. TAMSULOSIN 0.4 MG PO HS
SYP. ALKASTON B6 15 ML IN 1 GLASS WATER PO BD
GRBS 7 POINT PROFILE
INJ. HAI S/C TID
INJ. NPH S/C BD
SYP. POTKLOR 10 ML IN GLASS OF WATER PO TID



Comments
Post a Comment